
Five years after the pandemic began, a haunting question remains: Why do millions suffer long after the virus has cleared? A compelling new hypothesis suggests that SARS-CoV-2 acts as a master key, unlocking ancient viruses, latent bacteria, and genetic “ghosts” that have been hiding within us all along.

The war against COVID-19 was supposed to have a clear beginning and end. It began in late 2019 in Wuhan, China, with a novel pathogen, and for most, it ended with the clearance of the virus from the body. Yet, for a staggering number of survivors, the “all clear” signal was a mirage. They remain trapped in the fog of Long COVID (Post-Acute Sequelae of SARS-CoV-2), battling symptoms ranging from debilitating fatigue and cardiac inflammation to cognitive decline.
For years, the scientific community has hunted for the direct cause. Is it a viral reservoir hiding in the gut? Is it persistent tissue damage? A comprehensive review from Rutgers New Jersey Medical School offers a more complex and unsettling answer. The study suggests that the devastation of Long COVID may not be caused solely by the coronavirus itself, but by a phenomenon known as “Immune Theft.”
The hypothesis is chilling in its simplicity: The sheer biological cost of fighting SARS-CoV-2 distracts the immune system so thoroughly that it stops watching the “prisoners” it has been guarding for years-reawakening dormant enemies ranging from Tuberculosis to ancient viral fragments embedded in our own DNA.
The Connection Between COVID-19 and SARS
The virus causing COVID-19 is named SARS-CoV-2 because of the ‘SARS’ epidemic that appeared in China in 2002-03. Both COVID-19 and SARS are respiratory diseases with similar effects. The causative virus of SARS, ‘SARS-CoV-1,’ shares structural and genetic similarities with the ‘SARS-CoV-2’ virus that causes COVID-19.
However, SARS-CoV-1 did not possess the ability to bind to our body’s cells as easily as its successor, SARS-CoV-2. Because the infection could be identified quickly that epidemic did not spread globally. The SARS outbreak at that time was limited to about ten thousand cases, resulting in approximately one thousand deaths.
SARS-CoV-2 possesses ‘Spike Proteins’ on its outer surface that can easily attach to our respiratory cells. Because of this capability, COVID-19 infection occurs more easily than SARS, and the probability of transmission from an infected person to others is also faster. For this reason, COVID-19 found the opportunity to spread to all continents of the world within a short time.
The Question of Long-Term Effects
In most people, COVID infection lasts for two to three weeks. After recovering from COVID, the SARS-CoV-2 virus is cleared from the body. However, just because our immune system removes the SARS-CoV-2 virus does not mean all effects of the infection are over. In some individuals, various problems continue to be seen for months after infection. These long-term effects of COVID-19 are termed ‘Long COVID.’
The causative virus of COVID-19, SARS-CoV-2, does not have the ability to hide and remain dormant in our bodies. If the virus itself is no longer present, research is ongoing to understand how its long-term effects persist. In this context, a study recently released by researchers at Rutgers University has raised a significant question: Could COVID-19 be reactivating other infections already hiding inside the body to cause Long COVID?
Structure of SARS-CoV-2 and Viral Entry
The COVID-19 seen in most of us begins after the SARS-CoV-2 virus infects the cells of the respiratory system. This virus can enter the body through the nose, mouth, or eyes via aerosols- microscopic droplets released when an infected person coughs, sneezes, or speaks.
Upon reaching the body, the virus’s first choice is the lungs and cells related to the respiratory system, the surfaces of which are abundant in a protein called the ‘ACE2 Receptor.’ In normal conditions, the ACE2 receptor assists cells in external signaling and biological regulation processes. However, during COVID-19, the SARS-CoV-2 virus utilizes this very ACE2 receptor as the main doorway for entry.
SARS-CoV-2 is a type of RNA virus. Just as we store our genetic information in the DNA of our chromosomes, some viruses store this information in RNA. SARS-CoV-2 does not have DNA, nor does it need it. Their genome, or genetic material, consists of ‘positive-sense RNA’ located at the center of the virus. ‘Positive sense’ means that once they enter the host cell, they can use the cell’s machinery to easily produce viral proteins. SARS-CoV-2 does not need to enter the host cell’s nucleus or create new DNA or additional RNA at the very beginning.
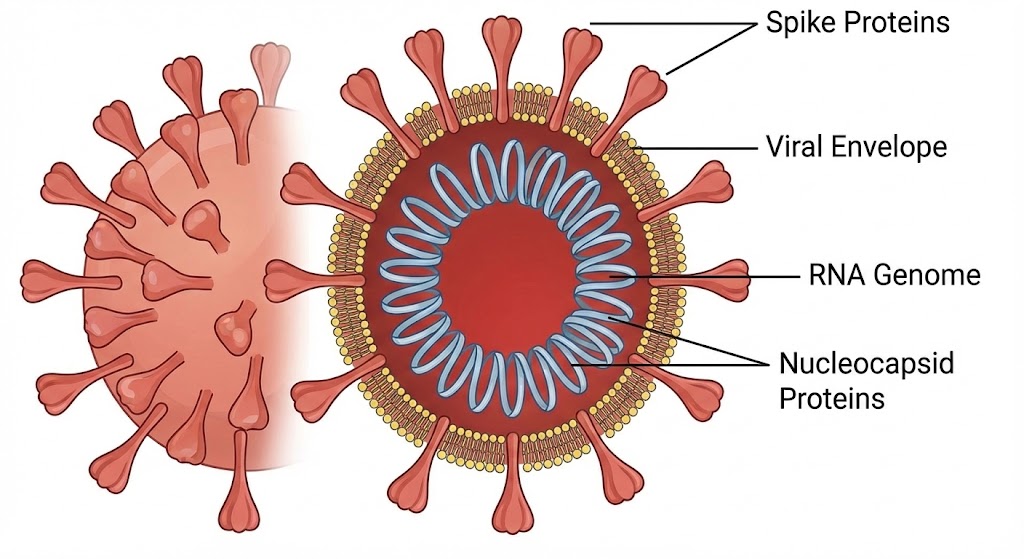
The outer covering of the SARS-CoV-2 virus is covered by a viral envelope made of lipids, which protects the virus. Soap and water, alcohol, or hand sanitizers destroy the virus by affecting this very layer. The membrane inside the viral envelope consists of three types of proteins: Spike, Membrane, and Envelope proteins. Among these, the Membrane and Envelope proteins provide structural protection to the virus. At the center of the virus is the RNA, which is surrounded and protected by the Nucleocapsid protein.
The Spike Protein and the Start of Infection
The Spike protein is the most important for SARS-CoV-2 infection. The name ‘Coronavirus’ is derived from this feature. Resembling a crown (Latin: Corona) on the outer surface, these spike proteins are of two types: Spike-1 and Spike-2. Spike-1 functions to attach to the host cell’s ACE2 receptor, while Spike-2 helps fuse the virus and the host cell membrane together. Compared to SARS-CoV-1, the Spike protein of SARS-CoV-2 attaches much more easily and strongly to the host cell’s ACE2 receptor. It is due to this characteristic that COVID-19 was able to spread across the world much more easily and quickly than SARS.
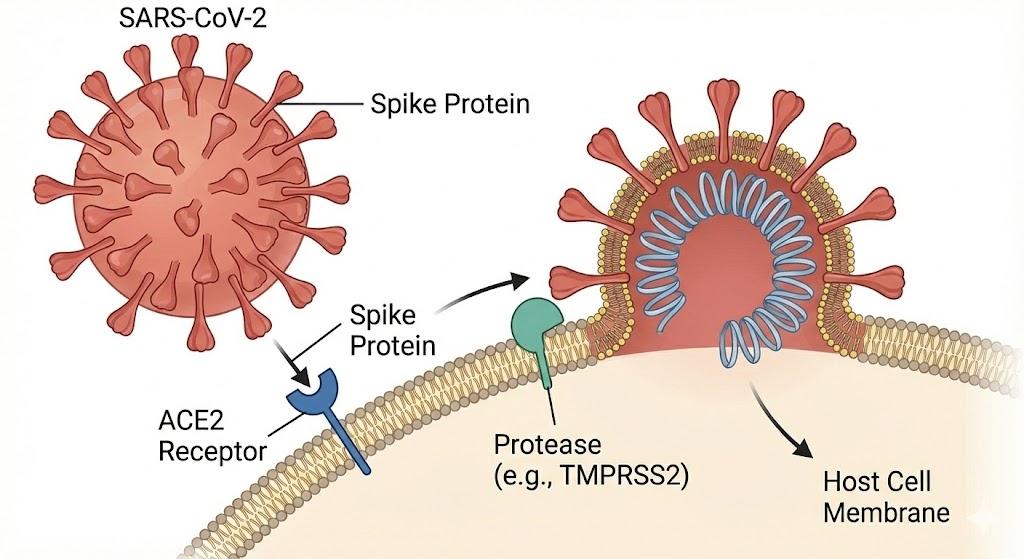
Once the virus’s Spike protein binds to the host cell’s ACE2 receptor, a protease (protein-cutting) protein called ‘TMPRSS2’ present inside the cell becomes active. Acting like scissors, it cuts a part of the Spike protein, activating viral entry and opening the path for viral RNA to enter the host cell.
In cases where TMPRSS2 is insufficient or if the virus has mutated, the viral genome can also enter the host cell through another process called ‘Endocytosis.’ The virus and the ACE2 receptor combine to form a small, round structure called an ‘Endosome,’ through which the virus enters the cell. The ‘Omicron’ variant, which appeared after mutations in the original Wuhan virus, primarily infected cells through this process.
The Viral Replication Process
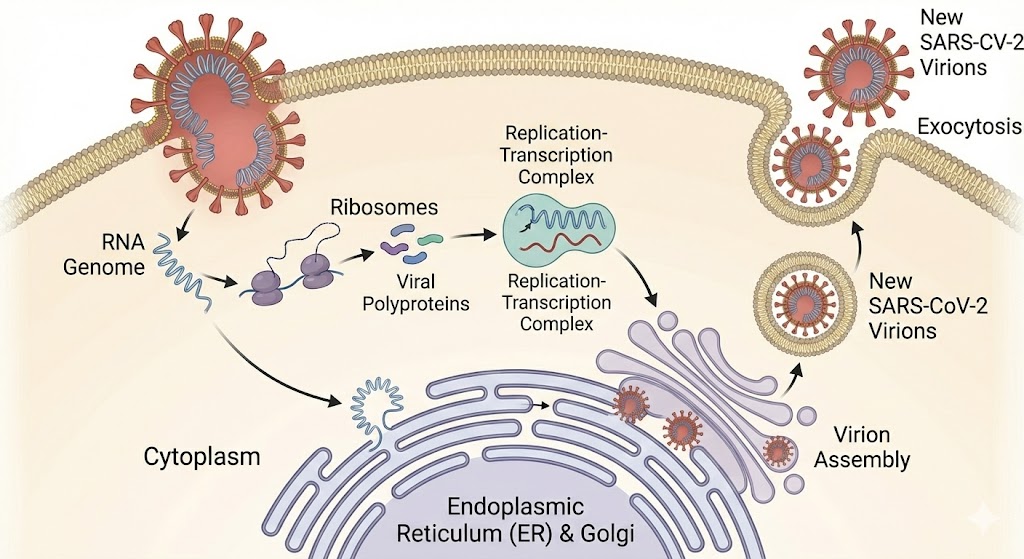
Since SARS-CoV-2 RNA is ‘positive-sense,’ once it reaches the host cell’s cytoplasm, it immediately acts as messenger RNA (mRNA) to start the protein production process. The viral RNA initially uses the host cell’s ribosomes to create the virus’s non-structural proteins. There are sixteen of these proteins, and at the start of infection, they are the virus’s main weapons. Non-structural proteins disrupt the host cell’s biological processes and divert them toward replicating the virus. At the start of infection, they create special structures within the host cell that suppress the body’s initial immune response and help accelerate the viral replication process.
The replication process of the SARS-CoV-2 virus differs from many other viruses. The replication of its RNA occurs entirely within the host cell’s cytoplasm. This virus never enters the cell nucleus and does not have the ability to integrate with our DNA in any way. As soon as infection occurs, the newly formed proteins create special structures within the host cell, the membranes of which shield the viral RNA and the replication process from the body’s immune system.
This process, which begins as soon as the virus reaches the cytoplasm, is rapid and occurs on a war footing. The viral replication process starts after an enzyme called ‘RNA-dependent RNA polymerase’ begins making a reverse (negative anti-sense) copy of the RNA. Using that as a template, multiple copies of the forward (positive-sense) RNA-identical to that found in the new virus-are prepared. Some of these RNAs are used to make proteins, while others are used as the genome for new viruses.
As infection and replication proceed, host cells essentially turn into virus-producing factories. The normal functions of infected cells are gradually suppressed. The energy, amino acids, and ribosomes of the infected cells are spent solely on making new viruses. These cells eventually die, but not before producing a massive number of new viruses. The newly formed viral particles exit the infected cells and spread the infection to nearby cells.
The Body’s Defense: War and Damage
COVID-19 infection presents a dilemma for our body. When infection starts, the body’s ‘Innate Immune System’ (initial defense system) recognizes the viral proteins and RNA and can produce cytokines, including ‘Interferons,’ to fight the virus. If the immune system identifies the virus early and removes it quickly, one may survive severe infection. The vaccines we use generally function for this purpose. However, SARS-CoV-2 has the ability to suppress this initial Innate Immune System.
Once the virus begins infecting respiratory cells, it can make many copies at once. As new viral copies start attacking nearby cells, the severe effects of COVID begin to appear. The infection becomes complex, and the body’s ‘Adaptive Immune System’ activates to join the fight.
When the adaptive immune system starts fighting COVID, severe effects appear in some individuals. In some, cytokine imbalance, blood vessel damage, and blood clotting processes begin, which can lead to ‘Acute Respiratory Syndrome’ and ‘Organ Failure.’ This can be understood as follows: becoming critically ill from COVID-19 is the equation of the effects of both the virus and the immune system fighting against it.
If our adaptive immune system works, the viral load gradually decreases. After the infection ends, SARS-CoV-2 residues cannot remain in the body for long, nor does this virus have the ability to hide in cells or DNA. In almost everyone who recovers, viral RNA is not present in the body 14 to 21 days after infection.
Here, the main question puzzling science is this: When the virus has disappeared from the body and the PCR report is negative, why does the body not signal that the war is over?
Long COVID: Why Do Problems Persist After Recovery?
SARS-CoV-2 has unique capabilities that may have brought about various changes in the body. The condition where problems arise later due to changes that occurred during the active infection is called ‘Long COVID,’ or in medical language, ‘Post-Acute Sequelae of SARS-CoV-2’ (PASC).
The symptoms of Long COVID are quite bizarre and vary from person to person. Some feel extreme fatigue, while others experience ‘Brain Fog’-clouding of the mind, loss of concentration, and difficulty thinking. After the active SARS-CoV-2 infection ends, viral fragments or RNA have been found remaining in some cells other than the respiratory system, such as the gut, brain, or other tissues. Hiding in small amounts for some time, these can cause continuous inflammation. Similarly, dead viral fragments may remain in the body, and the immune system may attack them, thinking they are active viruses. This is one reason for persistent sweating or continuous fatigue long after COVID has ended.
In some, a serious problem of heart muscle inflammation called ‘Myocarditis’ is seen. The acute infection of COVID also damages blood vessels. ‘Micro-clotting’ of blood occurs in vessels, obstructing oxygen delivery to various organs. This is found in many who have trouble breathing and fatigue for a long time. While damage to lung or heart tissues takes a long time to heal, there is also a risk of an ‘Autoimmune Response,’ where the immune system loses its way and attacks its own healthy cells.
The Rutgers Study: The Theory of ‘Immune Theft’
There is another possibility-when the body’s entire immune system is focused on the battle against the Coronavirus, it loses surveillance over other ‘dormant’ viruses and bacteria suppressed within the body for years. Consequently, just as prisoners escape when prison guards are removed, these old infections or ‘criminals’ get a chance to raise their heads again. This study suggests that the cause of Long COVID may not just be the residue of the Coronavirus, but ‘hidden enemies’ reawakened by the body’s weakened immune state.
A comprehensive review published by researchers at Rutgers New Jersey Medical School in the journal ‘eLife’ questions this very possibility. Could this unbalanced state of the body’s immunity be the breeding ground for ‘Long COVID’? Their conclusion suggests that some serious symptoms of Long COVID are not caused by the SARS-CoV-2 virus itself. They indicate in their review paper that due to ‘Immune Hijacking’ or deviation in our immune system during the fight against infection, these permanent but dormant viruses, bacteria, and other ‘Dark Antigens’ may have reactivated.
Residues of Old Diseases Hidden in DNA
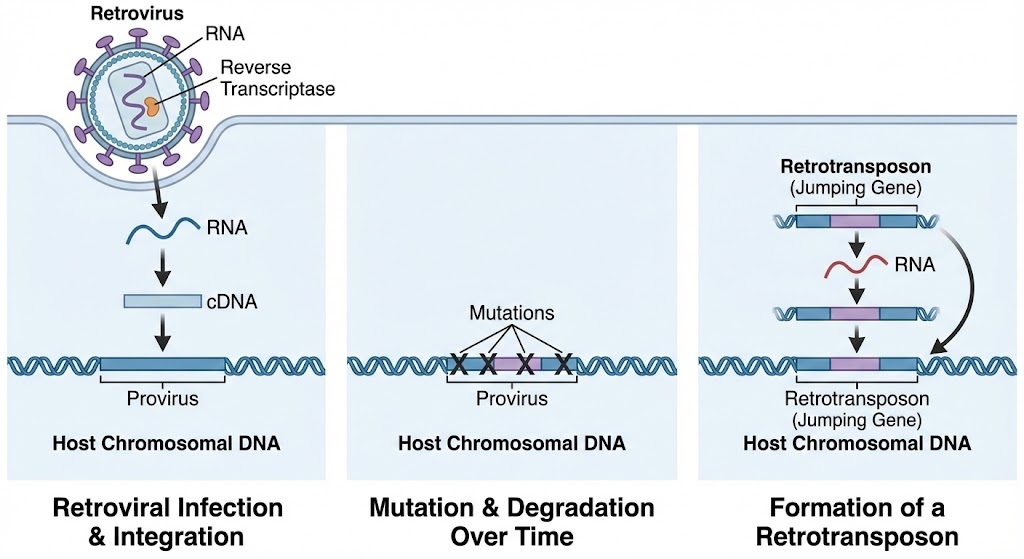
If we turn the pages of our DNA and view chromosomes as a biography, we find that the early chapters are written by viruses. A large part of our DNA is made of residues of these ancient infections-fragments of prehistoric retroviruses, broken viral enzymes, and scattered genetic husks that once replicated with ruthless efficiency.
Some viruses or bacteria have developed the ability to hide inside DNA. For example, retroviruses like HIV, which causes AIDS, have viral DNA that can hide in our chromosomes for a lifetime and be passed down to new generations. Residues of ancient retroviruses that infected our bodies have made a permanent home in our DNA as ‘Transposons’ or ‘Jumping Genes.’
Some bacteria or viruses can enter the cell nucleus and use its replication machinery but cannot integrate into the DNA. Some respiratory viruses have this ability. Certain viruses (like EBV, CMV) and bacteria (like TB), while unable to do both, suppress the ability to make their proteins to avoid immune surveillance and have developed the ability to hide in various cells and remain in our bodies for a lifetime.
As mentioned at the beginning of this article, the COVID-19 virus does not have such capability, but its infection may have brought about many changes. First, the virus has the ability to cause ‘Remodeling’ of chromatin in immune cells even before severe infection. To put it simply, the virus can change how the ‘Instruction Manual’ inside the cell is read or used. Such immune remodeling caused by the virus may leave long-term effects on the immune system. In a sense, COVID-19 is not just a respiratory disease, but also a disease of the immune system.
Chromatin remodeling causes an imbalance in cytokines, leaving a long-term obstruction in the development of ‘Monocytes’ that recognize viruses, or ‘T’ and ‘B’ cells that fight them. Even if SARS-CoV-2 residues are removed from the body, the ‘Transcriptional’ (process of making RNA and protein from DNA) functions changed during infection remain distorted-as if the immune system has learned the wrong lesson and cannot forget it.
Immune Distraction: War at the Border, Insecurity in the City
Another aspect of the long-term effects of COVID-19 is the body’s immune system. During a complex, acute COVID-19 infection, a state of biological emergency exists within our body. As soon as SARS-CoV-2 attacks, the entire immune mechanism-especially ‘T-cells,’ ‘B-cells,’ and ‘Natural Killer cells’-leave their other duties and focus on the ‘Frontline’ of the lungs and respiratory system. After COVID-19 infection, the immune system is weakened; soldiers are either killed in the war or are extremely exhausted.

It is here that a major lapse occurs in the body’s security system during the fight against SARS-CoV-2. In scientific terms, this is called ‘Immune Distraction.’ Let’s understand it this way: Suppose the country’s entire army is busy fighting a foreign enemy (Coronavirus) at the border. At such a time, the internal security of the capital and other cities becomes weak, and hidden internal enemies get a chance to rise. It is exactly the same in our body. This study questions whether the danger of long-term effects is not due to the external enemy, SARS-CoV-2, but due to the reawakening of ancient viral residues that have been sleeping in our bodies for thousands of years.
Thus, while the immune system unites to fight against COVID, ‘Immune Surveillance’-the process of constant vigilance in the body-weakens. The Rutgers study calls this ‘Immune Theft’ by COVID. This creates a large hole in the security mechanism. It is through this hole that ‘hidden enemies’ take advantage-such as latent Tuberculosis, Retroviruses, Herpes virus, or Epstein-Barr virus. ‘Lymphopenia,’ a deficiency of white blood cells seen in COVID patients, further encourages this security void.
About 8 percent of our DNA consists of such ancient retroviral residues, which infected our ancestors millions of years ago and later became part of our genome. Normally, our body keeps them silent by applying an ‘Epigenetic’ lock. However, the Immune Theft created by COVID-19 infection can break those locks. Consequently, these ancient viruses or ‘Transposons’ become active and start making their proteins. In this state, the immune system considers these proteins made from its own DNA as ‘foreign’ and starts attacking. The study points out a strong possibility that some autoimmune problems seen in Long COVID-where the body attacks its own healthy organs-could be due to the reactivation of these ‘Dark Antigens.’
Hidden Enemies: Tuberculosis and Other Viruses
Retroviruses have the ability to integrate into DNA and be passed down, but many other hidden enemies could hide in the body waiting for an opportunity to reactivate. Among these ‘hidden enemies,’ the reactivation of Epstein-Barr Virus (EBV) and Cytomegalovirus (CMV) has made Long COVID symptoms even more mysterious. About 95 percent of adults worldwide are infected with EBV. Similarly, CMV infection is found in 85 percent of people. Our immune system recognizes and easily removes this infection in childhood. However, a small amount of the virus may reduce its power to make new viruses and hide in the body for a lifetime. In normal conditions, the immune surveillance keeps these small amounts of virus suppressed.
When the immune system fights hard against COVID-19, immune surveillance elsewhere in the body weakens, giving these hidden opportunistic viruses a chance to raise their heads. As the Rutgers study shows, when COVID-19 degrades the function of immune soldiers (T, B, and Natural Killer cells), EBV can reawaken. This might be why the rate of patients visiting hospitals due to reactivated EBV has been increasing by ten percent annually post-pandemic. The ‘Brain Fog,’ extreme fatigue, and neurological weaknesses felt by Long COVID patients correspond largely to symptoms of active EBV. Similarly, when CMV activates, it causes inflammation in blood vessels and works to age the overall immune system prematurely (‘Immune Aging’). Because of this, people in their 30s and 40s begin to feel fatigue and weakness typical of 60 or 70-year-olds.
For a country like Nepal, the most worrying subject is the activation of ‘Latent Tuberculosis’ (TB). In a large portion of our population, TB bacteria are locked inside small nodules in the lungs called ‘Granulomas.’ Due to the excessive inflammation caused by COVID-19, there is a risk that the structure of these nodules holding the bacteria may be destroyed. Like prisoners escaping after prison walls collapse, these bacteria begin to spread in the lungs.
The problem becomes more complex here-symptoms of active TB and Long COVID, such as prolonged cough, evening fever, weight loss, and extreme fatigue, are largely similar. This leads to the possibility of patients and doctors mistaking it for ‘normal post-COVID effects’ or just ‘Long COVID.’ If health problems are visible for a long time after COVID, this study forces us to think seriously that it might not just be the effect of the virus, but TB reawakened by COVID. Therefore, when managing Long COVID patients in Nepal, it now seems mandatory to prioritize TB testing as well.
The Final Insult: Immune Amnesia
As if reawakening old enemies wasn’t enough, COVID-19 may also erase our defenses against them. The Rutgers review touches on the concept of “Immune Amnesia.”
Much like a computer hard drive being formatted, a severe infection can wipe the body’s “memory banks.” Research suggests COVID-19 can destroy Memory B-cells and antibodies accumulated over a lifetime. This means the biological lessons we learned from childhood vaccines or past flus could be lost. Survivors may find themselves inexplicably vulnerable to common pneumonias and pathogens they should have been immune to.
A New Paradigm for Treatment
The implications of the “Immune Theft” hypothesis are transformative. If Long COVID is indeed driven by the reactivation of dormant threats, then treating it solely as a sequel to the coronavirus is a mistake.
We are not just dealing with the footprint of a virus that has left the building; we are dealing with the riot it incited before it left. The medical community must broaden its diagnostic lens. Treating Long COVID may require screening for reactivated EBV, managing latent TB, and stabilizing the immune system to put the “Dark Antigens” back to sleep.
COVID-19 has taught us a harsh lesson: We are never truly alone. We carry a history of biological battles within us, and it only takes one key to unlock them all.

Leave a comment